by Lauren Earhart
In the early nineteenth century, the US slave trade was a major economic driver. Owning healthy, hard-working slaves was considered to be among the most important forms of capital. Additionally, having fertile slaves that could birth and produce more slaves for posterity was vital in order to keep the slave market alive. This became especially true after the ban on non-domestic slave trade in 1808.1 As the demand for slave labor increased, owners began to show increased interest in the reproductive health of their female slaves. This, combined with doctors’ interest in medical experimentation and their need for research subjects, led to unethical gynecological practices on enslaved women.
As the slave economy grew, the Deep South became a breeding ground for experimental hospitals seeking the next medical innovation. Doctors chasing fame and fortune exploited the maladies experienced by enslaved people in order to establish and perpetuate their medical reputations. Dr. Paul Eve was one such doctor; in 1850 in Augusta, Georgia, he conducted the first successful complete hysterectomy in the US. The surgery was performed on a young slave named Mary, who had complained of vaginal bleeding and infertility for the majority of her life. Dr. Eve, a renowned surgeon in the South, diagnosed the young woman with cancer and formed a team to excise the cancer. When Mary died three months after the surgery, she did not understand that the surgery rendered her infertile and, therefore, devalued in the eyes of her owners and husband. Mary never got the full story of her surgery, and died without ever understanding the risks Dr. Eve had imposed on her against her will. Dr. Eve never took responsibility for his actions, writing, “The history of diseases among our negro population is generally very imperfect and unsatisfactory, and this is especially true as regards uterine derangements.”2

Dr. Ephraim McDowell, the “Father of the Ovariotomy,” which is the surgical removal of one or both ovaries, also owed much of his success to dark, unethical medical practices. After successfully performing an ovariotomy on a white woman, McDowell sought out more subjects to practice his surgical technique on. Not surprisingly, these surgical subjects were enslaved women. Remarkably, in the early 1800s, he was able to locate four slaves with ovarian tumors in the small town of Danville, Kentucky for surgical practice. As Dr. McDowell gained notoriety, Black community members began to fear him. McDowell developed a reputation for causing harm and death in his Black patients without ever truly experiencing any repercussions. As stated by his granddaughter, Mary Young Riddenbaugh, “The negroes of the village and the surrounding country being naturally ignorant and superstitious, whenever they spied Dr. McDowell walking in the distance, would rush into the nearest building, fearing that he might waylay and maltreat them. They feared him as they would some beast of prey.” McDowell’s work advanced the field of gynecology, but the slaves he worked on suffered through painful, unethical surgeries in order to make this happen. However, McDowell’s peers still discredited his techniques and the sacrifice of the enslaved women by stating, “Negresses . . . will bear cutting with nearly, if not quite, as much impunity as dogs and rabbits.”2
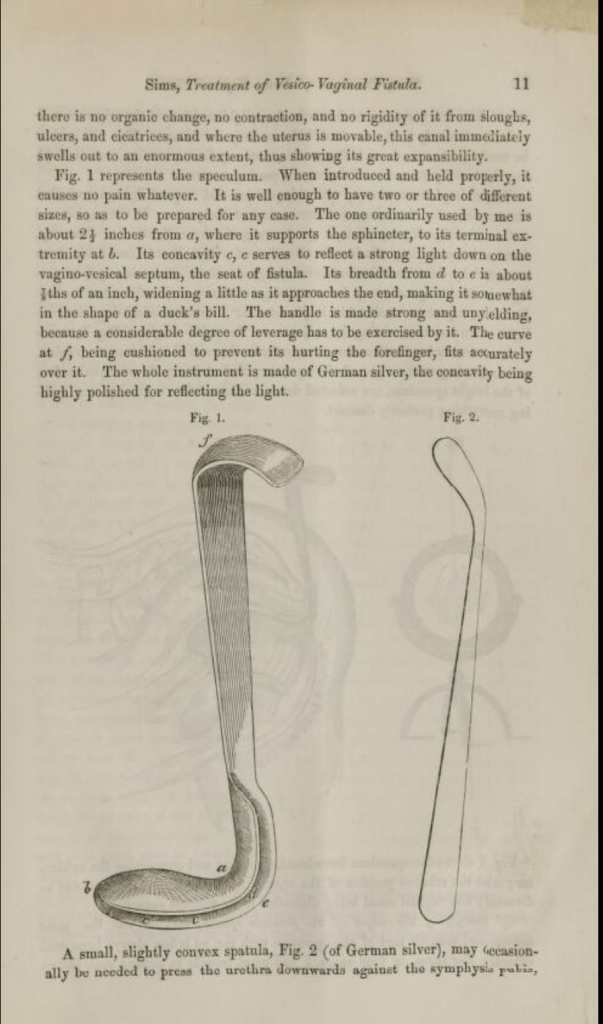
On the Treatment of Vesico-Vaginal Fistula by
Dr. James Marion Simsb.
The most famous pioneer of gynecology was perhaps the most unethical and cruel. Dr. James Marion Sims, also known as “The Father of Modern Gynecology,” gained prestige and fame from his work in developing the vaginal speculum (a tool used to examine the vaginal canal and cervix) and a surgical technique for repairing vesicovaginal fistulas. A vesicovaginal fistula occurs when an opening develops between the bladder and vagina, and it often occurs as a result of difficult labor during childbirth. This medical condition was common in female slaves, and was of special interest due to slave owners’ desire to have their slaves in optimal reproductive health. Upon moving to Alabama, presumably to secure a steady supply of test subjects and chase medical renown, Dr. Sims opened a crude hospital on his own property dedicated to perfecting his surgical techniques on enslaved women. He devoted nearly five years of his career to experimenting on these poor, defenseless women.2 We only know the name of three women: Lucy, Betsy, and Anarcha. He subjected Anarcha to approximately thirty surgeries over the course of these five years. At the time of her first surgery, Anarcha was only 17 years old.1 Anarcha’s story was played out again and again for the other thirteen slaves Dr. Sims housed at his primitive hospital, all enduring grueling surgeries until the day Sims finally created a successful technique for treating vesicovaginal fistulas.
Even more horrifying, Dr. Sims rarely utilized anesthesia during his surgeries on slaves, even though it was available and an accepted surgical practice at the time. Other medical practitioners of the time followed a similar anti-anesthesia philosophy for treating Black patients. This was rooted in the prejudiced belief that Blacks were capable of enduring more pain than whites. It was a common belief that Blacks had thicker skulls, thicker skin, and less sensitive nervous systems compared to other races.1 These beliefs provided false moral justification to the decision to withhold anesthesia and perpetuated the unethical and cruel medical practices conducted on female slaves.
Unfortunately, many of the prejudiced beliefs and practices experienced by female slaves persist in today’s society. Studies have found that many medical practitioners are prone to underestimate the pain experienced by their Black patients.5 In 2016, a study found that approximately forty percent of first- and second-year medical students endorsed the idea that Blacks have thicker skin than whites. Stemming from these beliefs, an analysis over 20 years of research revealed that Black patients were 22% less likely to receive pain medication than white patients in a variety of settings.3 Additionally, infant mortality rates are 2.3 times higher in Black populations compared to non-Hispanic white populations. This fact is especially ironic, given that the bodies of Black women were sacrificed to advance the fields of obstetrics and gynecology. Not surprisingly, these past abuses have led to a legacy of distrust between the Black community and the still largely white medical profession. As put by authors Dr. Dierdre Owens and Dr. Sharla Fett, “How does a community learn to trust doctors whose forefathers were interested only in repairing and restoring Black women’s reproductive health so that slavery could be perpetuated?”4

The impacts of the unethical gynecological practices on enslaved women still reverberate today. The field of gynecology was advanced at the expense of these women; without the experimentation they endured, innovations in diagnostic and curative techniques would not be nearly as advanced as they are today. Therefore, the field of gynecology owes both an apology and debt to the often nameless Black women who sacrificed their bodies and minds to endure the cruel practices of white doctors. Mary, Anarcha, Lucy, Betsy, and the countless other women need to be acknowledged for their contributions and involuntary participation in unethical experimentation. To this day, a hospital is named after Dr. Ephraim McDowell, with their slogan claiming “Excellence is Our Only Standard.” After becoming the president of the American Medical Association, Dr. James Marion Sims had a statue erected in his honor in New York, which was only recently tore down in 2018. Perhaps instead of giving these unethical men credit and recognition, we should name hospitals and build statues that honor the sacrifices of the women they experimented on. In order to reconcile the disparities and improper distribution of recognition, understanding the history of the field of gynecology is essential. True equality in medical treatment for the Black community and other People of Color can not be achieved until the historical roots of biases and prejudices are identified and acknowledged.
References
- Bachynski, K. (2019, April 1). Perspective | American medicine was built on the backs of slaves. And it still affects how doctors treat patients today. The Washington Post. https://www.washingtonpost.com/news/made-by-history/wp/2018/06/04/american-medicine-was-built-on-the-backs-of-slaves-and-it-still-affects-how-doctors-treat-patients-today/.
- Owens, D. C. THE BIRTH OF AMERICAN GYNECOLOGY. In Medical Bondage Race, Gender, and the Origins of American Gynecology (pp. 15–41). essay, University of Georgia Press.
- Sabin, J. A. (2020, January 6). How we fail black patients in pain. AAMC. https://www.aamc.org/news-insights/how-we-fail-black-patients-pain.
- Owens, D. C., & Fett, S. M. (2019). Black Maternal and Infant Health: Historical Legacies of Slavery. American Journal of Public Health, 109(10), 1342–1345. https://doi.org/10.2105/ajph.2019.305243
- Hoffman, K. M., Trawalter, S., Axt, J. R., & Oliver, M. N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences, 113(16), 4296–4301. https://doi.org/10.1073/pnas.1516047113
Image Sources
a. First Ovariotomy: Onondaga Historical Association. https://www.cnyhistory.org/2020/05/the-first-ovariotomy/ (Public Domain).
b. On the treatment of vesico-vaginal fistula: Archive.org. https://archive.org/details/67130240R.nlm.nih.gov/page/n7/mode/2up (Public Domain).
c. James Marion Sims, Father of Modern Gynecology: Thomas Hawk. https://www.flickr.com/photos/51035555243@N01/50232839381 (Public Domain).
d. NYC – Central Park – J. Marion Sims: Wally Gobetz. https://www.flickr.com/photos/70323761@N00/786104189 (Public Domain).